Quiz
PET/CT- Oncology
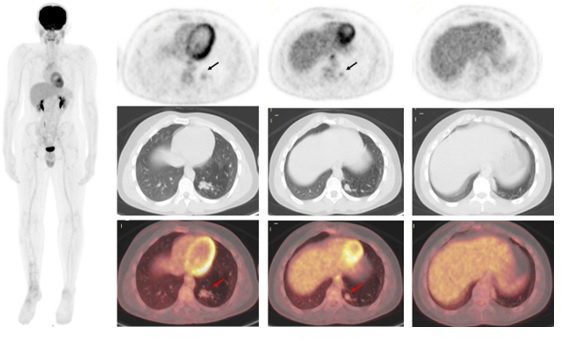
18-year-old male, a known case of right tibia osteosarcoma underwent surgical resection in 2021 followed by adjuvant chemotherapy. 18F-FDG PET/CT is performed for restaging. Whole body FDG PET/CT showed mild diffuse FDG uptake around the right tibial prosthesis (post-surgical changes). Note is made for mild to moderate focal increase FDG uptake at the medial basal segment of the left lung, lower lobe (arrow).
Click on thumbnails for larger images.
- Findings are suspicious for lung metastases as osteosarcoma often spreads to the lungs with an incidence of lung metastases of around 10-20%.
- Need further evaluation with HRCT for better characterization as the uptake is not very high
- Biopsy is suggested as it is characterized as high risk on Fleischner criteria.
- The mass is a well-defined, round, or ovoid lesion; slightly lobulated on computed tomography (CT). Findings are suggestive of carcinoid tumor. 68Ga-DOTA NOC can be advised for the evaluation of somatostatin receptor expression.
- No need for any further evaluation as it is a normal variant.
Scroll for answer
Answer 5
Discussion
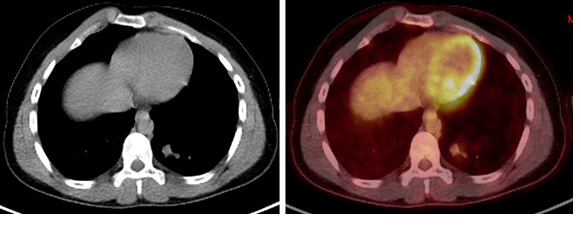
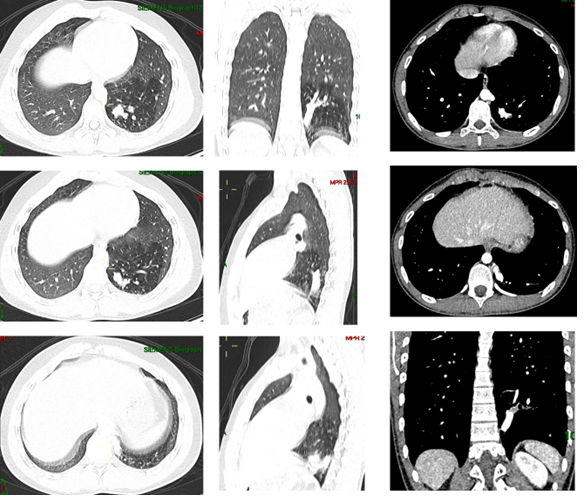
There is hyperlucent lung parenchyma in the medial and basal segment of the left lower lobe supplied by a tortuous artery arising from the descending thoracic aorta above the level of the diaphragm with mild to moderate FDG uptake similar to aorta. Findings are suggestive of Anomalous systemic arterial supply to normal segments of the lung.
CT section from CTPA at the level of inferior pulmonary veins shows a nipple-like structure with enhancement similar to that of descending thoracic aorta at the mediastinal edge of the left basal lung segments. This is an aberrant artery arising from the descending thoracic aorta. This pattern of origin of the aberrant artery from descending thoracic aorta and supply to the basal segment of the ft lower lobe is a rare congenital anomaly. The etiology of systemic arterial supply to normal lung is still unknown, it is generally believed that this might result from an abnormal persistence of the embryonic connection between aorta and pulmonary parenchyma [[i]]. This disease was previously classified as Pryce Type I sequestration [[ii]]. However, the absence of parenchymal abnormalities with a normal bronchial supply distinguishes systemic arterial supply from true pulmonary sequestration. [[iii]]. Most patients are asymptomatic, but patients might develop localized pulmonary hypertension, hemoptysis, and eventually high output cardiac failure which is likely related to the higher systemic arterial pressure compared with the normal lower pulmonary arterial pressures [[iv],[v]]. Contrast-enhanced CT is the preferred imaging method as it can identify the origin of anomalous systemic artery and can also assess the pulmonary arteries, tracheobronchial tree, and lung parenchyma [[vi]]. 18F-FDG PET is commonly used in diagnostic staging, restaging, and response evaluation in cancer patients; however, these findings are nonspecific for cancers and can also be found in inflammatory/infectious and normal variant conditions [[vii],[viii]]. Knowledge of this potential pitfall on 18F-FDG PET is important. Although an anomalous systemic arterial supply to normal lung is uncommon, it is important to increase awareness among nuclear physicians and radiologists to enable timely diagnosis and avoid unnecessary additional investigations for the patients.
[i]. Kirks DR, Kane PE, Free EA, et al. Systemic arterial supply to normal basilar segments of the left lower lobe. AJR Am J Roentgenol. 1976;126:817–821.
[ii]. Pryce DM. Lower accessory pulmonary artery with intralobar sequestration of lung; a report of seven cases. J Pathol Bacteriol. 1946;58:457–67
[iii]. Savic B, Birtel FJ, Tholen W, et al. Lung sequestration: Report of seven cases and review of 540 published cases. Thorax. 1979;34:96–101.
[iv]. Brühlmann W, Weishaupt D, Goebel N, Imhof E. Therapeutic embolization of a systemic arterialization of lung without sequestration. Eur Radiol. 1998;8:355–358
[v]. Bhalla AS, Gupta P, Mukund A, Kumar A, Gupta M. Anomalous systemic artery to a normal lung: a rare cause of hemoptysis in adults. Oman Med J. 2012;27:319-322.
[vi]. Do KH, Goo JM, Im JG, et al. Systemic arterial supply to the lungs in adults: spiral CT findings. Radiographics 2001; 21: 387–402.
[vii]. Fletcher JW, Djulbegovic B, Soares HP, et al. Recommendations on the use of 18F-FDG PET in oncology. J Nucl Med. 2008;49:480–508.
[viii]. Stumpe KD, Dazzi H, Schaffner A, et al. Infection imaging using whole-body FDG-PET. Eur J Nucl Med. 2000;27:822–832.