Neurology Case 1
You are here: > Teaching Cases and Quiz >> Neurology Case 1
Neurology Case 1
Submitted by :
Dr. Harmandeep Singh
MD MICNM FANMB
Assistant Professor
Department of Nuclear Medicine
PGIMER
Chandigarh
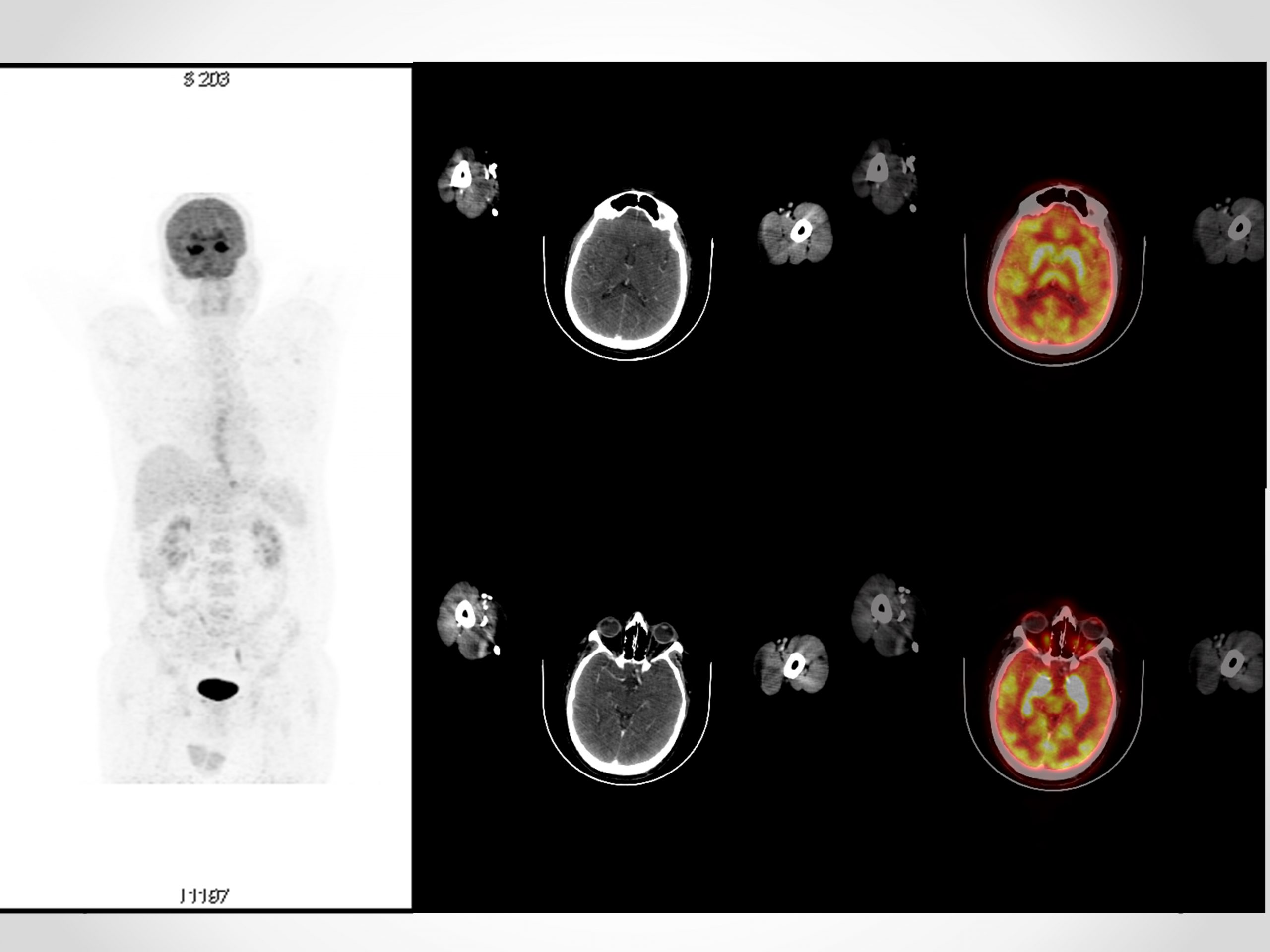
A 55 years old male presented with chief complaints of abnormal body movements, irrelevant talking and Behavioural abnormalities for 1 day. He had fever upto 104 degree Fahrenheit one week prior to this episode which was relieved with antipyretics. During hospital admission, he had 2 episodes of complex partial seizures, fluctuating sensorium and disorientation. Cranial nerve examination was normal, Tone was normal and Power 5/5 in all 4 limbs and plantar reflexes were bilateral flexor +. Sensory examination was normal and MMSE was 20/30. Recent memory was impaired. CSF examination revealed 10 cells per mm3 (predominantly lymphocytes), Protein 28 mg/dl and sugar 84 mg%. Autoimmune encephalitis, paraneoplastic encephalitis panel, viral markers, hematology, CSF and biochemistry work up were negative. Clinical Diagnosis of limbic encephalitis was made, with probable autoimmune or viral etiology. Initial MR was normal. 18F-FDG PET-CT was performed.
(Click on the image for full size)
Questions
What is the Probable Diagnosis based on 18F-FDG PET-CT findings?
- Mesial Temporal Sclerosis
- Limbic encephalitis
- Advanced Alzheimer’s
Disease - Creutzfeldt Jacob Disease
Scroll down for answer and discussion
Answer: B (Limbic Encephalitis)
Symmetrical hypermetabolism was noted in bilateral hippocampal region and basal ganglia. In view of symmetrical limbic system involvement, findings are suggestive of limbic encephalitis. Possible differentials include autoimmune and viral encephalitis.
Further Management:
CEMRI brain done after 2 days of 18F-FDG PET-CT revealed B/l hippocampal and mesial temporal lobe T2/FLAIR hyperintensity.
With likely diagnosis of Autoimmune Encephalitis, Rituximab therapy was planned for Immunomodulation. During the hospital stay, he regained partial insight. Repeat MRI revealed resolution of diffusion restriction and edema through signal changes persisted.
Discussion
95% energy for brain is obtained from glucose metabolism and is directly related to neuronal activity. This characteristic is basis of utility of 18F-FDG PET-CT in dementia, movement disorders and tumors.
In a normal 18F-FDG brain PET, homogenous symmetrical distribution is noted in brain with grey matter having 2.5-4 fold higher activity than white matter. Visual Cortex, Frontal eye fields and posterior cingulate cortices have higher uptake than other cortices whereas mesial temporal lobe has lower uptake as compared to other cortices. Basal ganglia show higher activity as compared to Neocortex.
Alzheimer’s Dementia, Mesial temporal sclerosis and CJD lead to hypometabolism in involved cortices.
Autopsy findings in Autoimmune Encephalitis have revealed Perivascular T cell infiltrates in messiah temporal lobes and basal ganglia. These can lead to higher FDG uptake in areas of active inflammation.
Diagnosis of Autoimmune encephalitis (AIE) is established when these 4 Criteria are met: 1. Subacute onset (rapid progression in <3 months) of memory deficits, seizures or psychiatric symptoms suggesting limbic system involvement. 2. Bilateral brain abnormalities on T2-W FLAIR MRI highly restricted to medial temporal lobes. 3. CSF pleocytosis (WBC >5 cells/mm3) or EEG with epileptic / slow wave activity involving temporal lobes. 4. Reasonable exclusion of alternate causes. Detection of antibodies can establish the diagnosis if one of first 3 criteria are not met. 18F-FDG PET-CT can be used to fulfil the second criterion.
Common reported 18F-FDG PET findings in AIE include Temporal, Orbito-frontal and basal ganglia hypermetabolism. Hypometabolism in Parietal and Occipital cortices has also been reported. Likely cause of hypometabolism are direct blockade of receptors or ion channels by autoantibodies which may lead to a decrease in neuronal and synaptic activity. 18F-FDG PET has been shown to be more sensitive and can detect inflammation even in cases with normal MRI.
References
- Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016 Apr; 15(4): 391–404.
- Tripathi M, Tripathi M, Roy SG,et al. Metabolic topography of autoimmune non-paraneoplastic encephalitis. Neuroradiology. 2018 Feb;60(2):189-198.