Osteology case 4
July 31st, 2020
Dr. Sharjeel Usmani.
KBNM, FEBNM, FANMB, MS, CBNC.
Specialist Nuclear Medicine.
Kuwait Cancer Control Center
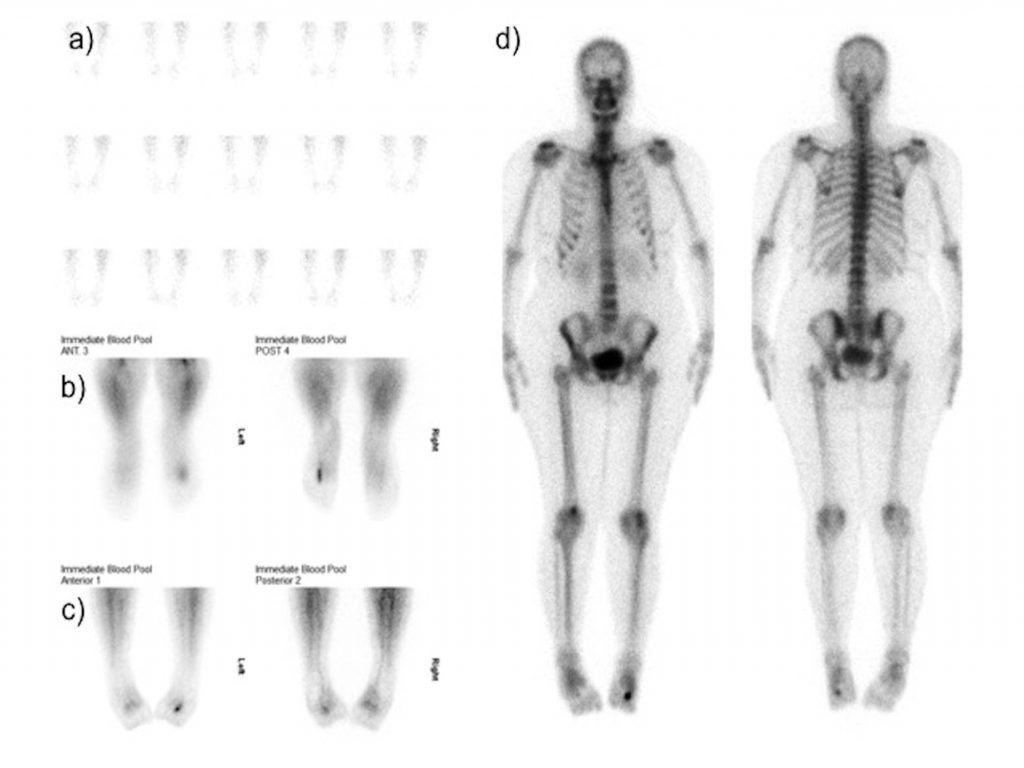
51-years old female presented with severe pain at the dorsum of left foot. Clinical examination shows severe tenderness. No history of prior trauma, fracture and no sign of inflammation and redness. a-c) Flow and blood pool images show increase flow and hyperemia at left distal foot region. d) Delayed images show intense tracer uptake at head of 3rd metatarsal bone. What is the diagnosis ?
- Osgood schlatter disease
- Köhler disease
- kienbock disease
- Frieberg’s disease
Scroll down for correct answer.
Correct answer:
4 – Frieberg’s disease
Positive three phase bone scan at head of 3rd metatarsal bone. Findings are likely due to spontaneous avascular necrosis (Frieberg’s disease).
Freiberg disease is avascular necrosis of the metatarsal head primarily affecting the second or third metatarsal bone [[i]]. Symptoms include swelling, limited range of motion, and tenderness of the affected foot. The diagnosis of Freiberg disease is confirmed with X-rays. Radiography show sclerosis and widening of the joint space (early), with complete collapse of the metatarsal head and fragmentation later. Bone scintigraphy with Tc-99m MDP shows photopenia in the early stages of the disease and intense uptake in the head later during the healing revascularized phase [[ii]]. Magnetic resonance imaging (MRI) is helpful in detecting early Freiberg disease not visualized on plain radiographs. MRI may demonstrate hypointense signal in the epiphysis on T1 images and mixed hypointense and hyperintense signals on T2 images [[iii]]. Treatment of Freiberg disease includes corticosteroid injections, immobilization, and orthotics.
Kienbock disease is an aseptic avascular necrosis of lunate bone unrelated to acute fracture. Clinically presented as pain and stiffness in the wrist with associated swelling and tenderness dorsally over the radio-lunate joint [[iv]].
Kohler disease is a childhood avascular necrosis of the navicular bone. Radiographically appeared as wafer-like, fragmented navicular bone demonstrating patchy sclerosis, often associated with soft tissue swelling [[v]]. The age at presentation is between 2 and 10 years, with boys more likely to be affected than girls. Radiographs show increased sclerosis and sometimes flattening and fragmentation of the navicular.
Osgood-Schlatter disease (OSD) is a condition in which the patellar tendon insertion on the tibial tuberosity becomes inflamed [[vi]]. It usually affecting boys between ages 10-15 years. It is characterized by pain over the tibial tuberosity along with a bony prominence [[vii]].
References:
[i]. Shane A, Reeves C, Wobst G, Thurston P. Second metatarsophalangeal joint pathology and freiberg disease. Clin Podiatr Med Surg. 2013; 30:313-325.
[ii]. Mandell GA, Harcke HT. Scintigraphic manifestations of infraction of the second metatarsal (Freiberg’s disease). J Nucl Med. 1987;28:249-51.
[iii] . Mifune Y, Matsumoto T, Mizuno T, et al. Idiopathic osteonecrosis of the second metatarsal head. Clin Imaging. 2007;31:431-3.
[iv]. Horch RE, Unglaub F, Dragu A, et al. Kienböck’s disease. Diagnosis and therapy. J Am Acad Orthop Surg. 2008;79:452–60.
[v]. Haller J, Sartoris DJ, Resnick D, et al. Spontaneous osteonecrosis of the tarsal navicular in adults: imaging findings. AJR Am J Roentgenol. 1988; 151: 355-8.
[vi]. Hyphenated history: Osgood-Schlatter disease. Nowinski RJ, Mehlman CT. Am J Orthop (Belle Mead NJ). 1998;27:584–585.
[vii]. Rosenberg ZS, Kawelblum M, Cheung YY, et al. Osgood-Schlatter lesion: fracture or tendinitis? Scintigraphic, CT, and MR imaging features. Radiology. 1992;185:853-8.