PET Basics 2
PET Basics 2
Uploaded on Ocober 1st, 2020
By Dr. Riffat Parveen Hussain.
Consultant Nuclear Medicine Physician.
Department of Radiology.
Section of PET CT.
Jinnah Postgraduate Medical Centre.
Karachi
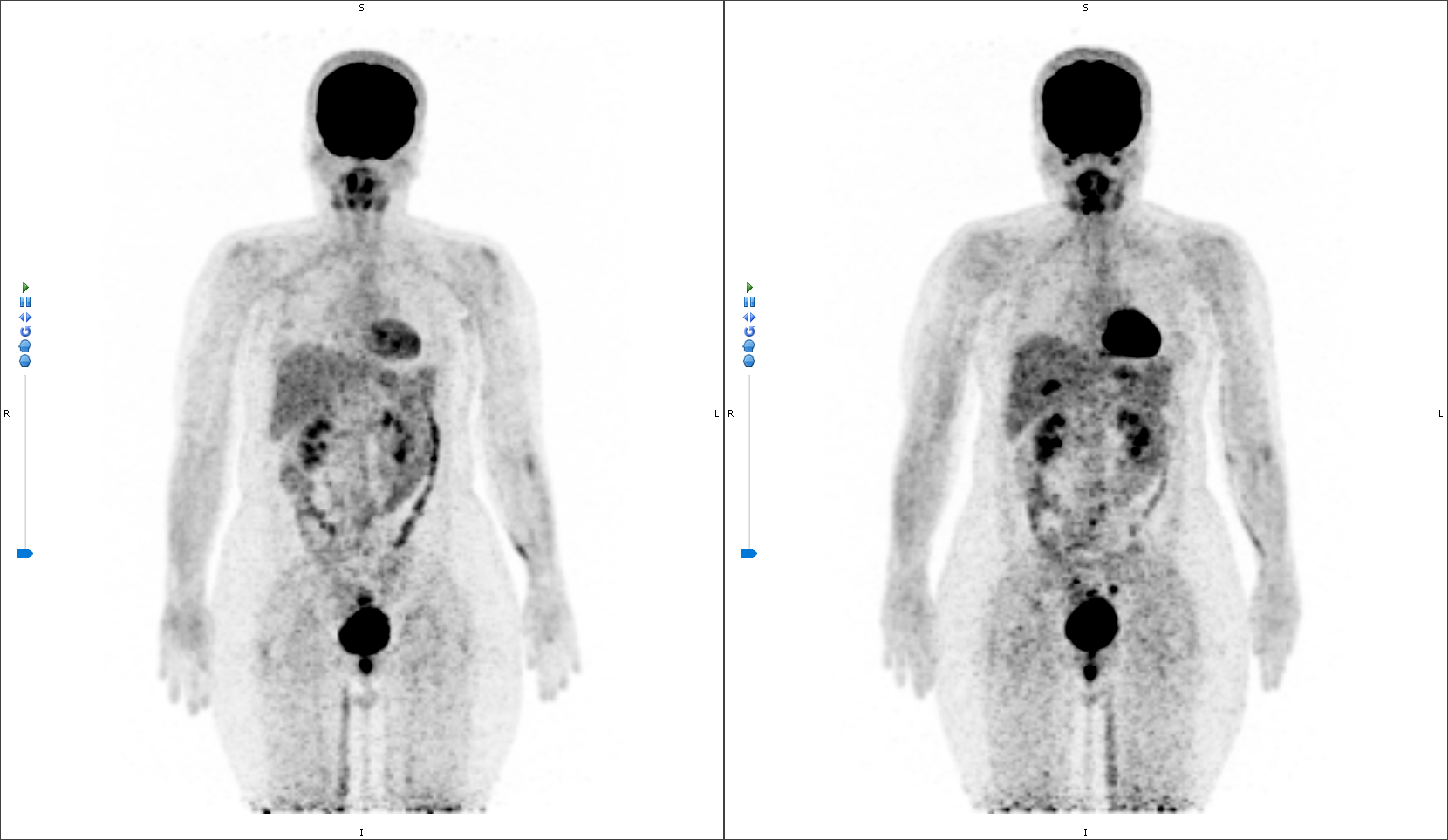
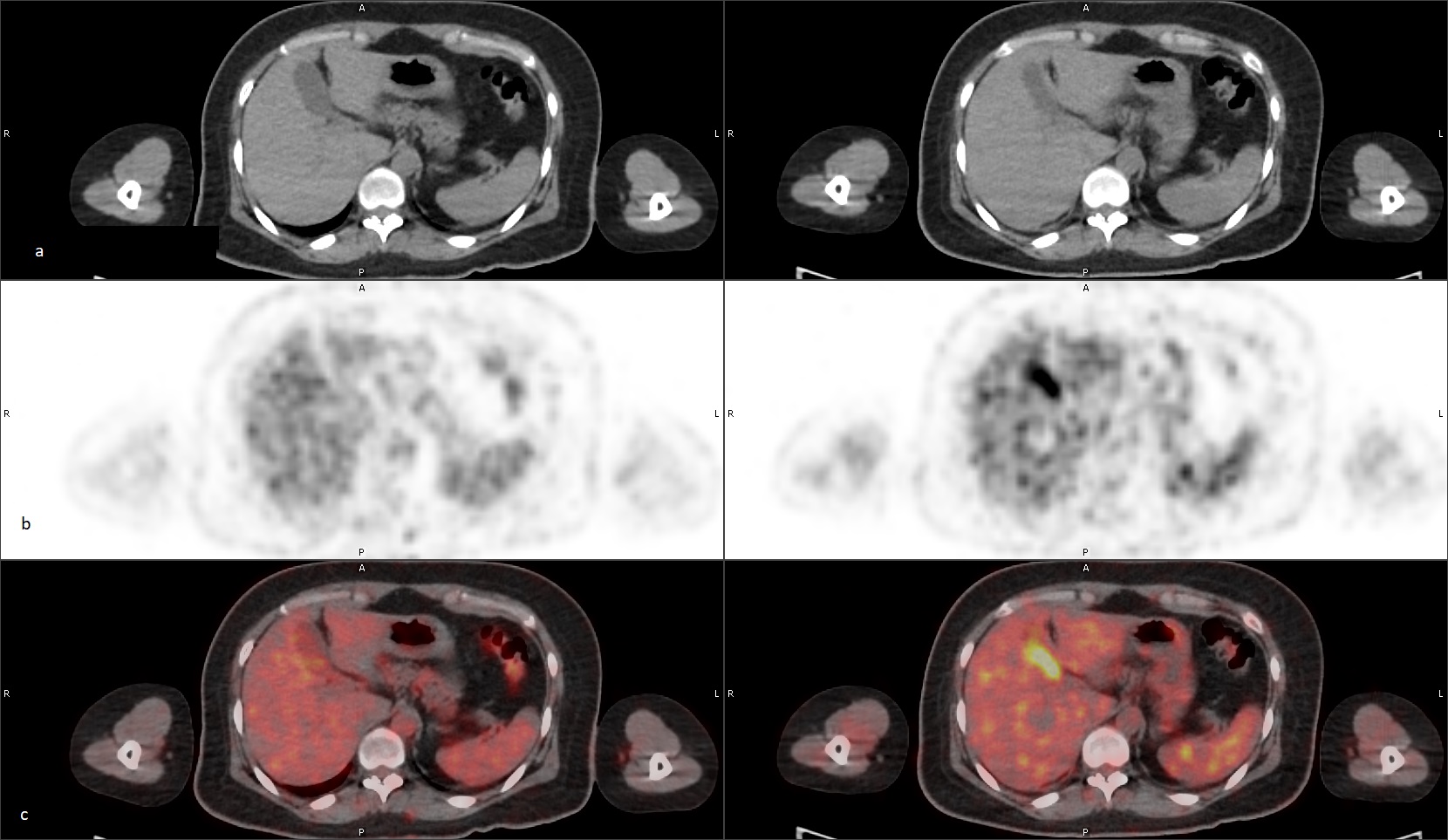
A 42-year-old female, diagnosed case of carcinoma right breast, status post mastectomy and chemotherapy, underwent 18F FDG PET scanning for the evaluation of treatment response. Present scan showed an interval development of increased metabolic activity overlying gall bladder (GB). The concomitant CT images failed to show any anatomical/morphological abnormality in the region.
Ultrasound of the region showed an adequately distended GB with no evidence of abnormality or pathology. Laboratory workup, inclusive of liver profile, was all within the normal limits and the patient gave no history of any complaints related to GB.
What is the most likely cause/diagnosis: –
- Acute cholecystitis
- Adenocarcinoma Gall Bladder
- Gall bladder polyp
- Gallbladder adenomyomatosis
- Normal Physiological uptake

These images were published as a case report (Ref 2).
Scroll down for correct answer and discussion
Correct answer is:
5. Normal physiological uptake
Discussion
The GB in the FDG PET‑CT studies, normally, does not show any tracer accumulation(1,2).
Reports in literature, however, have noted the accumulation of tracer despite the absence of any GB disease which sometimes have been higher than the activity of the liver. It is important to be cognizant of this physiology as it will help in not incorrectly attributing the uptake to a pathological cause (1–3). Discussion of each stem given as below: –
- Adenocarcinoma Gall Bladder
GB uptake in the face of known malignancy of the organ is well known with adenocarcinoma of GB being the most common (4,5). On PET‑CT, a malignancy of the GB shows a diffuse increased tracer uptake with abnormal CT findings such as a morphological massive tumor or wall thickening (4).
- Acute cholecystitis
In addition to the clinical symptoms, acute cholecystitis usually produces a ring-like uptake of FDG. This pattern is quite different from that produced by physiological accumulation; thus, acute cholecystitis and physiological GB accumulation are usually easy to differentiate on PET/CT (1).
- Gallbladder adenomyomatosis (6)
Gallbladder adenomyomatosis (GA) is a benign alteration of the gallbladder wall that can be found in up to 9% of patients. GA is characterized by a gallbladder wall thickening containing small bile-filled cystic spaces (i.e., the Rokitansky–Aschoff sinuses, RAS). It may involve the gallbladder according to four main patterns: localized, segmental, annular and diffuse.
Independent of the radiological modality, an imaging clue for diagnosing GA is the detection, within a thickened gallbladder wall, of Rokitansky–Aschoff sinuses. Consequently, ultrasound (US), the imaging modality of choice for the diagnosis shows either focal or diffuse GB wall thickening, mural reverberations or a constriction in the gallbladder circumference.
On the CT, gallbladder wall thickening without mural growth can be observed.
.
- Normal Physiological uptake
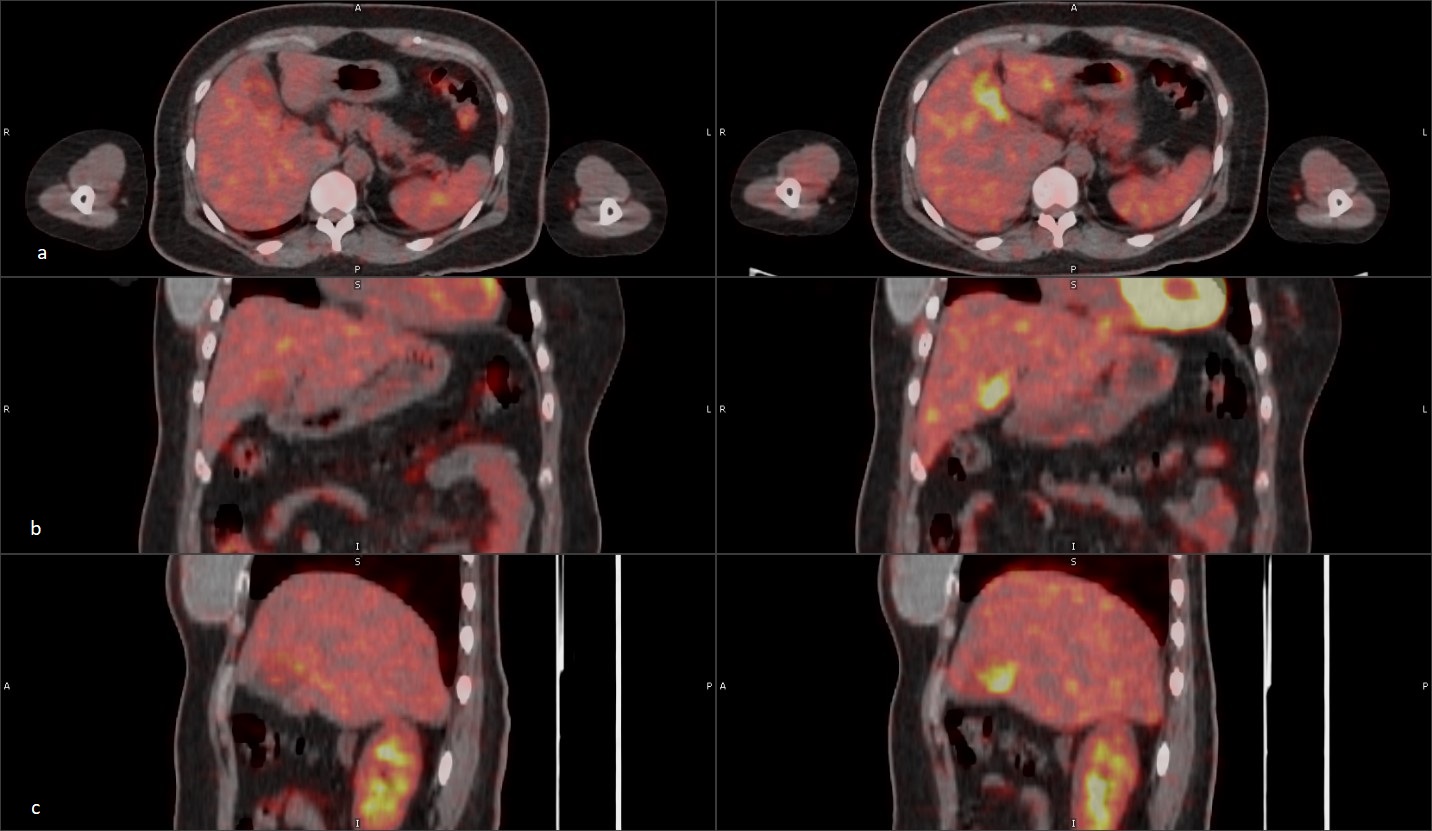
Normal physiological uptake of the GB, as was in this case, has also been described. Differentiating the physiological uptake from a malignant cause is usually not difficult as the former do not exhibit any abnormal CT findings such as a tumor or wall thickening, as usually seen for malignancy(2,7).
FDG appears, in the normal physiological conditions, to be distributed within the GB lumen and not the wall because it is secreted into the bile (1).
Another cause for tracer accumulation in the GB has been recognized in delayed imaging with the accumulation increasing with increase of time from injection(2,7).
- Gall bladder polyp
Gall bladder polyps are generally benign and show very little or no uptake of FDG tracer; if uptake is seen, it is used as a risk stratification for surgical intervention (8). They are mostly identified at US but are increasingly seen at computed tomography (CT) and magnetic resonance (MR) imaging (9).
References
- Murata Y, Watanabe H, Kubota K, Toda K, Nakamura S, Okouchi K, et al. PET/CT evaluation of the physiologic accumulation of 18F-FDG within the gallbladder vesicle. Nucl Med Biol [Internet]. 2007 Nov [cited 2019 Jun 12];34(8):961–6. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0969805107001862
- Hussain R, Nausheen S, Ahmed N, Mahmood T. Benign uptake of 18 F-fluorodeoxyglucose in the gallbladder on positron emission tomography-computed tomography. World J Nucl Med [Internet]. 2020;19(3):288. Available from: http://www.wjnm.org/text.asp?2020/19/3/288/290382
- Bai X, Wang X, Zhuang H. FDG Accumulation in the Lumen of the Gallbladder Without Related Pathology. Clin Nucl Med. 2018;43(5):383–5.
- Leung U, Pandit-Taskar N, Corvera CU, D’Angelica MI, Allen PJ, Kingham TP, et al. Impact of pre-operative positron emission tomography in gallbladder cancer. Hpb. 2014;16(11):1023–30.
- Maldjian PD, Ghesani N, Ahmed S, Liu Y. Adenomyomatosis of the Gallbladder: Another Cause for a “Hot” Gallbladder on 18 F-FDG PET. Am J Roentgenol [Internet]. 2007 Jul 23 [cited 2019 Jun 28];189(1):W36–8. Available from: http://www.ajronline.org/doi/10.2214/AJR.05.1284
- Bonatti M, Vezzali N, Lombardo F, Ferro F, Zamboni G, Tauber M, et al. Gallbladder adenomyomatosis: imaging findings, tricks and pitfalls.
- Rossi J, Mariluis CA, Delgado E, Choba R, Vietti CM. Pitfalls in Oncologic Diagnosis with PET CT . Nononcologic Hypermetabolic Findings. In: European Society of Radiology (EPOS)-ECR 2012. Vienna, Austria; 2012. p. 1–16.
- Lee J, Yun M, Kim KS, Lee JD, Kim CK. Risk stratification of gallbladder polyps (1-2 cm) for surgical intervention with 18F-FDG PET/CT. J Nucl Med. 2012;53(3):353–8.
- Mellnick VM, Menias CO, Sandrasegaran K, Hara AK, Kielar AZ, Brunt EM, et al. Polypoid lesions of the gallbladder: Disease spectrum with pathologic correlation. Radiographics. 2015;35(2):387–99.