Oncology case 1
April 14, 2020
Oncology Case 1
Dr. Senthil R, MD, FANMB, FEBNM.
Consultant & Head – Dept. of Nuclear Medicine & PET CT,
VPS Lakeshore Hospital & Research Centre,
Kochi – 682 040, Kerala, India.
Mobile: +91 9442366998
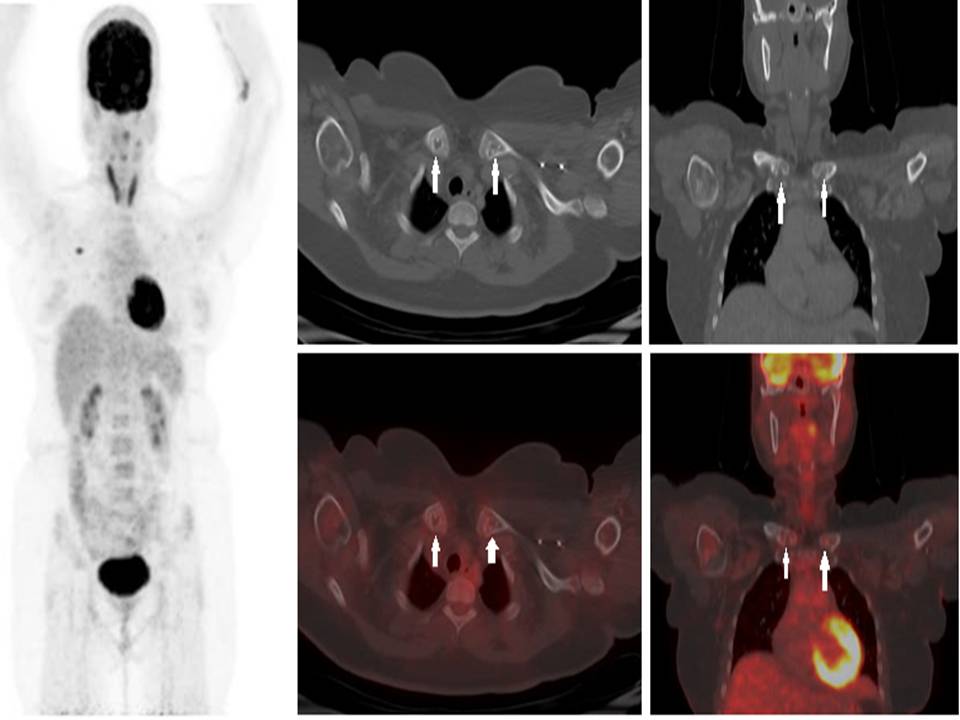
40 years old female, a recently diagnosed case of carcinoma of right breast underwent F-18 FDG PET CT for staging. It showed an FDG avid lesion in upper medial quadrant of right breast. In addition the following findings (white arrows) were seen in clavicles; what is the diagnosis?
- Skeletal metastases
- Osteomyelitis
- Rhomboid fossa
- Fossa ovalis
Scroll down for answers and discussion.
Answer:
3. Rhomboid fossa
Discussion
If a finding is bilateral and symmetrical, a probable anatomical/physiological should be considered possible. Usually lytic skeletal metastases from breast carcinoma are FDG avid and more commonly involve axial skeleton. Isolated lytic clavicular metastases occurring bilaterally without any FDG uptake is unlikely. (1)
Osteomyelitis
Even though osteomyelitis appears as lytic lesion on CT, it is usually FDG avid on PET and may be associated with abscess or soft tissue component. It is also unusual to occur as isolated bilateral symmetrical clavicular osteomyelitis (2).
Rhomboid fossa
Rhomboid fossa is normal depression along the inferomedial aspect of the clavicle, which is attachment site of the costoclavicular (rhomboid) ligament. It appears as osteolytic defect or irregularity on CT. It may also appear as a tuberosity. Its may be confused with pathological conditions like osteomyelitis or lytic metastasis, particularly during unilateral occurrence (3, 4).
Fossa ovalis
Fossa ovalis (Thigh) – otherwise known as saphenous opening is seen at the upper and medial part of the thigh, a large oval-shaped aperture in the fascia lata. It transmits the great saphenous vein, and other smaller vessels. (5)
Fossa ovalis (Heart) is an oval depression of interatrial septum, present toward the right atrium above and to the left of the orifice of inferior vena cava. (6)
References:
- O’Sullivan GJ, Carty FL, Cronin CG. Imaging of bone metastasis: An update. World J Radiol. 2015 28;7:202-11.
- Pineda C, Espinosa R, Pena A. Radiographic imaging in osteomyelitis: the role of plain radiography, computed tomography, ultrasonography, magnetic resonance imaging, and scintigraphy. Semin Plast Surg. 2009;23:80-89.
- De Wilde V, De Maeseneer M, Lenchik L, Van Roy P, Beeckman P, Osteaux M. Normal osseous variants presenting as cystic or lucent areas on radiography and CT imaging: a pictorial overview. Eur J Radiol. 2004;51:77-84.
- Paraskevas G, Natsis K, Spanidou S et al. Excavated-type of rhomboid fossa of the clavicle: a radiological study. Folia Morphol (Warsz). 2009;68:163-166.
- Gray, Henry. Anatomy of the Human Body. Page 469.
- Joshi SD, Chawre HK, Joshi SS. Morphological study of fossa ovalis and its clinical relevance. Indian Heart J. 2016;68:147-52.