Osteology Case 6
Osteology case 6
Uploaded on November 14th 2022
Dr. Afroza Naznin Akhee
MBBS, M Phil, FANMB
Senior Medical Officer & Asst. Professor
Institute of Nuclear Medicine & Allied Sciences, Mitford,
Dhaka, Bangladesh.
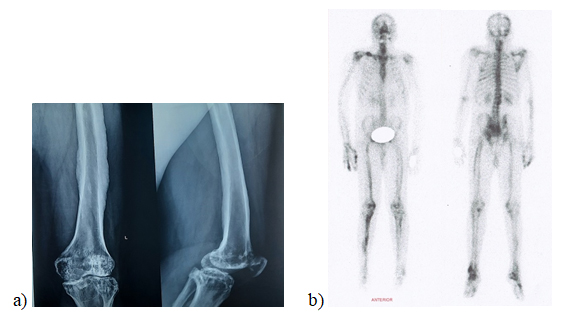
A 35 year old male presented with painful joint swelling since adolescence. He had no history of fever, trauma, change in skin color, or any other abnormality. Figure a) Plain radiograph showing cortical thickening with dripping wax appearance, b) Tc-99m bone scan revealing linear tracer accumulation at cortical regions in most of the long bones with absence of medullary activity. What is the diagnosis?
- Hypertrophic osteoarthropathy
- Melorheostosis
- Caffey disease
- Skeletal metastases
Scroll down for answer
Correct answer-
2. Melorheostosis
Melorheostosis is an atypical sclerosing bone dysplasia also known as candle bone disease or melting wax syndrome due to its characteristic dripping candle wax pattern of the affected bone cortex on X-rays. It can affect any age group with no gender predilection. It is usually asymmetrical, commonly affects unilateral long bones and sometimes tubular bones of hand and feet.Axial skeleton involvement can also be found rarely. Melorheostosis results in mild to moderately avid Tc-99m MDP accumulation in areas of sclerosis, possibly due to increased bone turnover or increased bone mass in the affected region.
Hypertrophic osteoarthropathy is characterized by symmetrical periosteal reaction of long bones, and almost always occurs in the setting of other systemic disease, inflammatory condition or malignancy.
Caffey disease or infantile cortical hyperostosis is a self-limiting disorder which presents within first five months of life. It commonly affects flat bones, though long bone involvement can also occur.
Sclerotic or osteoblastic skeletal metastasis is commonly found in prostate or breast carcinoma, and mostly affects axial skeleton.
References:
[1]. Wordsworth P, Chan M. Melorheostosis and osteopoikilosis: a review of clinical features and pathogenesis. Calcified tissue international. 2019 May;104(5):530-43.
[2]. Suresh S, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. Clinical radiology. 2010 Aug 1;65(8):593-600.
[3]. Kumar R, Sankhala SS, Bijarnia I. Melorheostosis–case report of rare disease. Journal of Orthopaedic case reports. 2014 Apr;4(2):25.
[4]. Teoh CC, Teoh SR, Chieng DC, Ang XY, Hassim MH. Polyostotic melorheostosis: approach to clinical evaluation and management. Open Journal of Orthopedics. 2019 Jul 22;9(7):137-44.
[5]. Chang CC, Chuang YW, Hsu CC, Lin CY, Huang YF, Chen YM, Tyan YC. Demonstration of melorheostosis on bone scan. International Journal of Radiation Research. 2019 Jul 1;17(3):513-7.
[6]. Zeiller SC, Vaccaro AR, Wimberley DW, Albert TJ, Harrop JS, Hilibrand AS. Severe myelopathy resulting from melorheostosis of the cervicothoracic spine: a case report. JBJS. 2005 Dec 1;87(12):2759-62.
[7]. Freyschmidt J. Melorheostosis: a review of 23 cases. European radiology. 2001 Feb;11(3):474-9.
[8]. Michiels I, Schaub T, Scheinzabach M. Melorheostosis, osteopoikilosis and ostiopathia striata. Their clinical significance and the value of scintigraphy in the differential diagnosis. Beitrage zur Orthopadie und Traumatologie. 1990 Jun 1;37(6):317-30.