Osteology Case 2
May 21, 2020
Case uploaded by:
Quiz.
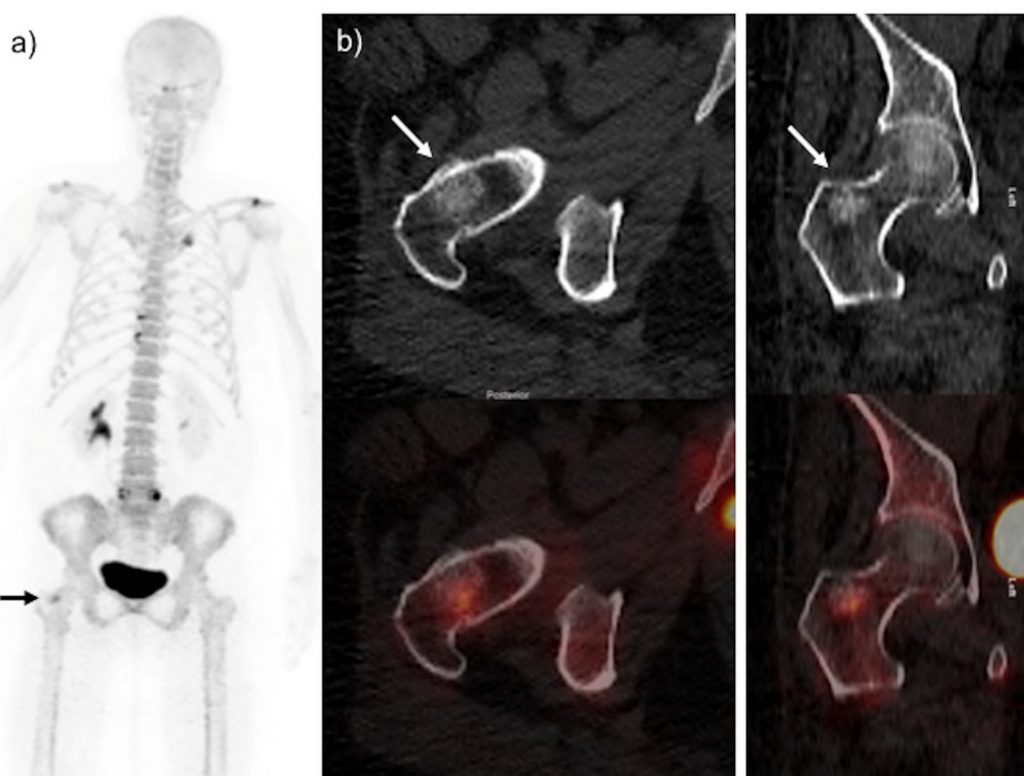
44-year old female with newly diagnosed breast cancer. 18F-NaF-PET/CT performed after injection of 4.3 mCi 18F-NaF for staging. a) MIP 18F-NaF image demonstrate degenerative/arthritic changes with increase osteoblastic activity at left acromioclavicular, sternoclavicular joints, osteophytes at D10-D11 and facets joints of L5/S1 vertebrae. b) Non-contrast axial and coronal CT images show sclerotic lesion at right trochanteric region with corresponding increased tracer activity on fused images (arrows). Solitary osteoblastic lesion at right trochanteric region with sclerotic changes on CT. What is the diagnosis ?
- Non-aggressive bone lesion at right trochanteric region, likely enchondroma; for follow-up.
- Non-aggressive bone lesion at right trochanteric region is likely benign, e.g Fibrous dysplasia; for follow-up.
- Findings consistent with sclerotic metastatic lesion; no further investigation needed.
- Aggressive solitary intramedullary osteoblastic bone lesion at right trochanteric region; for further radiological evaluation.
Scroll down for answer
Answer:
- Enchondroma
CT images show dense chondroid calcifications (in a rings and arcs pattern), with increased uptake on fused 18F-NaF PET/CT images. The lesion lacks aggressive features and most likely represents an enchondroma and follow-up scan is advised. It remains stable on follow-up imaging.
Enchondromas are benign intramedullary lesions composed of mature hyaline cartilage and comprising up to 15% of all benign bone tumors [[i]]. They are painless, with imaging features of endosteal scalloping less than two-third cortical thickness, absence of periosteal reaction or cortical breakthrough, and no associated soft tissue masses [[ii]]. It is usually solitary lesions in intramedullary bone occurring most commonly in small bones of the hands and feet but can be found in other long bones of the upper or lower limbs.
The typical CT features of enchondroma are “ring and arc” or “popcorn” chondroid matrix calcification, not penetrating to the cortex or extend into the soft tissues. These features may help to distinguish them from suspected metastases. Enchondromas may also show focal uptake on 99mTc MDP/18F-NaF and FDG PET/CT studies performed for cancer staging, resulting in a false-positive finding. If clinical suspicion is high, MRI and review by the bone tumor multi-disciplinary team should be considered, because biopsy, curettage, or both may be appropriate [[iii]].
18F-NaF PET-CT is a sensitive tool for detecting skeletal metastases surpassing conventional bone scintigraphy [[iv]]. Encouraging results are also seen in characterizing benign bone pathology [[v]]. Like conventional bone scintigraphy with 99mTc-MDP, 18F-NaF also accumulates in benign lesions due to increased bone turn over, which can mimic sinister pathology including metastases in oncology patients [[vi],[vii]]. In the literature, several benign conditions have been described with increased 18F-NaF accumulation for example inflammation and infection (osteomyelitis) [[viii]], past trauma [[ix]], fibrous dysplasia [[x]], Paget’s disease [[xi]], enchondroma [[xii]] osteonecrosis [[xiii]], and osteoid osteoma [[xiv]].
18F-NaF uptake in itself does not differentiate benign from malignant processes [[xv]]. The pattern of 18F-NaF uptake, however, may be suggestive (or in some cases for example rib fractures even characteristic) of a specific diagnosis. In this context correlation with morphological information from the CT and any other recent imaging is considered essential for diagnosis. 18F-NaF uptake in the benign bone lesions are not uncommon. The knowledge of these benign mimics is crucial, as misinterpretation can lead to unnecessary investigations and alter management. CT component is very useful for accurate localization and characterization of these benign mimics [[xvi]].
References
[i]. Dorman DD, Bogdan C. Bone Tumors. St. Louis, MO: Mosby; 1998.
[ii]. Murphey MD, Flemming DJ, Boyea SR, et al. Enchondroma versus chondrosarcoma in the appendicular skeleton: differentiating features. Radiographics. 1998;18:1213–1237.
[iii]. Döbert N, Menzel C, Ludwig R, et al. Enchondroma: a benign osseous lesion with high F-18 FDG uptake. Clin Nucl Med. 2002; 27:695–697.
[iv]. Löfgren J, Mortensen J, Rasmussen SH, et al. A Prospective Study Comparing 99mTc-Hydroxyethylene-Diphosphonate Planar Bone Scintigraphy and Whole-Body SPECT/CT with 18F-Fluoride PET/CT and 18F-Fluoride PET/MRI for Diagnosing Bone Metastases. J Nucl Med. 2017;58:1778-1785.
[v]. Ovadia D, Metser U, Lievshitz G, et al. Back pain in adolescents: assessment with integrated 18F-fluoride positron-emission tomographycomputed tomography. J Pediatr Orthop. 2007;27:90–3.
[vi]. Drubach LA. Clinical Utility of 18F NaF PET/CT in Benign and Malignant Disorders. PET Clin. 2012;7:293–301.
[vii]. Li Y, Schiepers C, Lake R, et al. Clinical utility of 18F-fluoridePET/CT in benign and malignant bone diseases. Bone. 2012;50:128–139.
[viii]. Strobel K, Fischer DR, Tamborrini G, et al. 18F-fluoride PET/CT for detection of sacroiliitis in ankylosing spondylitis. Eur J Nucl Med Mol Imaging. 2010;37: 1760–5
[ix]. Ovadia D, Metser U, Lievshitz G, et al. Back pain in adolescents: assessment with integrated 18F-fluoride positron-emission tomographycomputed tomography. J Pediatr Orthop. 2007;27:90–3.
[x]. Lee H, Lee KS, Lee WW. 18F-NaF PET/CT Findings in Fibrous Dysplasia. Clin Nucl Med. 2015 Nov;40:912-4.
[xi]. Installe J, Nzeusseu A, Bol A, et al. (18)F-fluoride PET for monitoring therapeutic re- sponse in Paget’s disease of bone. J Nucl Med. 2005;46:1650–8.
[xii]. Rohren EM, Macapinlac HA. Spectrum of Benign Bone Conditions on NaF-PET. Semin Nucl Med. 2017;47:392-396.
[xiii]. Dasa V, Adbel-Nabi H, Anders MJ, et al. F-18 fluoride positron emission tomography of the hip for osteonecrosis. Clin Orthop Relat Res. 2008;466:1081–6.
[xiv]. Strobel K, Vali R. (18)F NaF PET/CT versus conventional bone scanning in the assessment of benign bone disease. PET Clin. 2012;7:249–61.
[xv]. Sachpekidis C, Hillengass J, Goldschmidt H, et al. Quantitative analysis of 18F-NaF dynamic PET/CT cannot differentiate malignant from benign lesions in multiple myeloma. Am J Nucl Med Mol Imaging. 2017; 7: 148–156.
[xvi]. Usmani S, Ahmed N, Muzaffar S, et al. Spectrum of false positive 18F-sodium fluoride (NaF) bone PET/CT findings in Oncology imaging; A narrative pictorial review of cases from a single institution. Hell J Nucl Med. 2020;23:67-75.